


A breast cancer diagnosis is a life-altering event that brings an immediate whirlwind of medical appointments, scans, and treatment decisions. For younger women, this diagnosis often carries an additional, deeply personal layer of concern: “Will I still be able to have children?”
In recent years, medical statistics have shown a rising trend of breast cancer diagnoses among women in their 20s, 30s, and early 40s—years often dedicated to building a career or starting a family. The intersection of cancer care and reproductive health is a complex field known as oncofertility. While some breast cancer treatments can impact the ability to conceive, modern medicine offers more hope and more options than ever before.
Understanding the relationship between breast cancer treatment and fertility is essential for making informed decisions. Balancing the urgency of life-saving treatment with the dream of future parenthood requires a compassionate, multidisciplinary approach. This is where the expertise of a dedicated professional like Dr. Farah Arshad, a renowned Breast Cancer Specialist in Lucknow, becomes invaluable in guiding patients through these sensitive choices.
Breast cancer treatment can affect fertility depending on a woman’s age, ovarian reserve, and treatment type. However, fertility preservation options such as egg freezing and embryo freezing may help many women plan future pregnancies by protecting reproductive cells before treatment begins.
Understanding Fertility and Breast Cancer
Before diving into how treatments affect the body, it is important to understand how female fertility works. Women are born with a finite number of eggs stored in their ovaries, known as the ovarian reserve. Each month, hormonal signals prompt the ovaries to release an egg (ovulation).
Why Age Matters for Fertility
Age is the single most significant factor in a woman’s natural fertility. As women age, both the quantity and quality of their eggs decrease. When a woman undergoes breast cancer treatment, her “biological clock” may essentially be accelerated. A 30-year-old woman may have a better chance of recovering ovarian function after chemotherapy than a 40-year-old woman, simply because she starts with a larger ovarian reserve.
Why Breast Cancer Treatment Can Affect Reproductive Health
Fertility is a delicate hormonal balance. Many breast cancer treatments work by either killing rapidly dividing cells (chemotherapy) or blocking the hormones that fuel cancer growth (hormone therapy). Unfortunately, the ovaries are highly sensitive to these interventions. Damage to the eggs or the hormonal pathways can lead to temporary or permanent infertility.
Can Breast Cancer Treatment Cause Infertility?
The short answer is: It can, but it isn’t inevitable.
Infertility following treatment is often categorized into two types:
-
Temporary Infertility: Menstruation may stop during treatment (amenorrhea) but return months or even years after treatment ends.
-
Permanent Infertility: Treatment may cause the ovaries to stop functioning entirely, leading to premature menopause.
Factors That Influence Fertility Outcomes
Not every patient will experience the same impact on their reproductive health. The outcome depends on several variables:
-
Age at Diagnosis: Younger women generally have more resilient ovaries.
-
Ovarian Reserve: A baseline assessment of egg count (often via AMH blood tests) can predict risk.
-
Type of Treatment: Certain chemotherapy drugs are more “gonadotoxic” (toxic to the ovaries) than others.
-
Duration of Therapy: Longer treatment cycles increase the cumulative dose of medication, raising the risk of ovarian failure.

How Different Breast Cancer Treatments Affect Fertility
Each pillar of breast cancer care affects the reproductive system differently. To navigate this, patients must understand the specific risks associated with their prescribed regimen.
1. Chemotherapy and Fertility
Chemotherapy uses powerful drugs to destroy cancer cells. However, these drugs cannot always distinguish between a cancer cell and a healthy egg cell.
-
How it Affects Ovaries: Chemotherapy can damage or destroy primordial follicles (the sacs containing immature eggs) in the ovaries.
-
Risk of Early Menopause: If enough follicles are destroyed, the body enters “chemopause”—a state of premature menopause.
-
Fertility Recovery: Some women find their periods return within a year of finishing chemo, but the quality of their eggs may still be affected, making natural conception more difficult.
2. Hormone Therapy and Fertility
Many breast cancers are “hormone receptor-positive,” meaning they grow in response to estrogen or progesterone. To prevent recurrence, doctors prescribe hormone therapies like Tamoxifen or Aromatase Inhibitors.
-
Tamoxifen and Pregnancy: Tamoxifen is usually taken for 5 to 10 years. It is not safe to be pregnant while on Tamoxifen as it can cause birth defects. This means a woman may have to delay pregnancy until her late 30s or early 40s, by which time her natural fertility has naturally declined.
-
Ovarian Suppression: In some cases, doctors use injections (like Zoladex) to “shut down” the ovaries during treatment. While this is sometimes used to protect the ovaries, it also prevents pregnancy during the treatment window.
3. Radiation Therapy and Fertility
Radiation for breast cancer is typically targeted at the breast or chest wall.
-
The Good News: Because the radiation is focused far from the pelvis, it usually does not affect the ovaries or the uterus.
-
Rare Situations: In very rare cases of advanced or metastatic cancer where radiation is applied to the pelvic area or spine, the ovaries could be affected.
4. Surgery and Fertility
-
Breast Surgery: Lumpectomies and mastectomies do not affect the internal reproductive organs. However, they can impact a woman’s ability to breastfeed later on.
-
Ovarian Surgery: In women with high-risk genetic mutations (like BRCA1 or BRCA2), a Breast Cancer Specialist in Lucknow, might discuss the preventative removal of the ovaries (oophorectomy). This procedure results in immediate and permanent infertility.
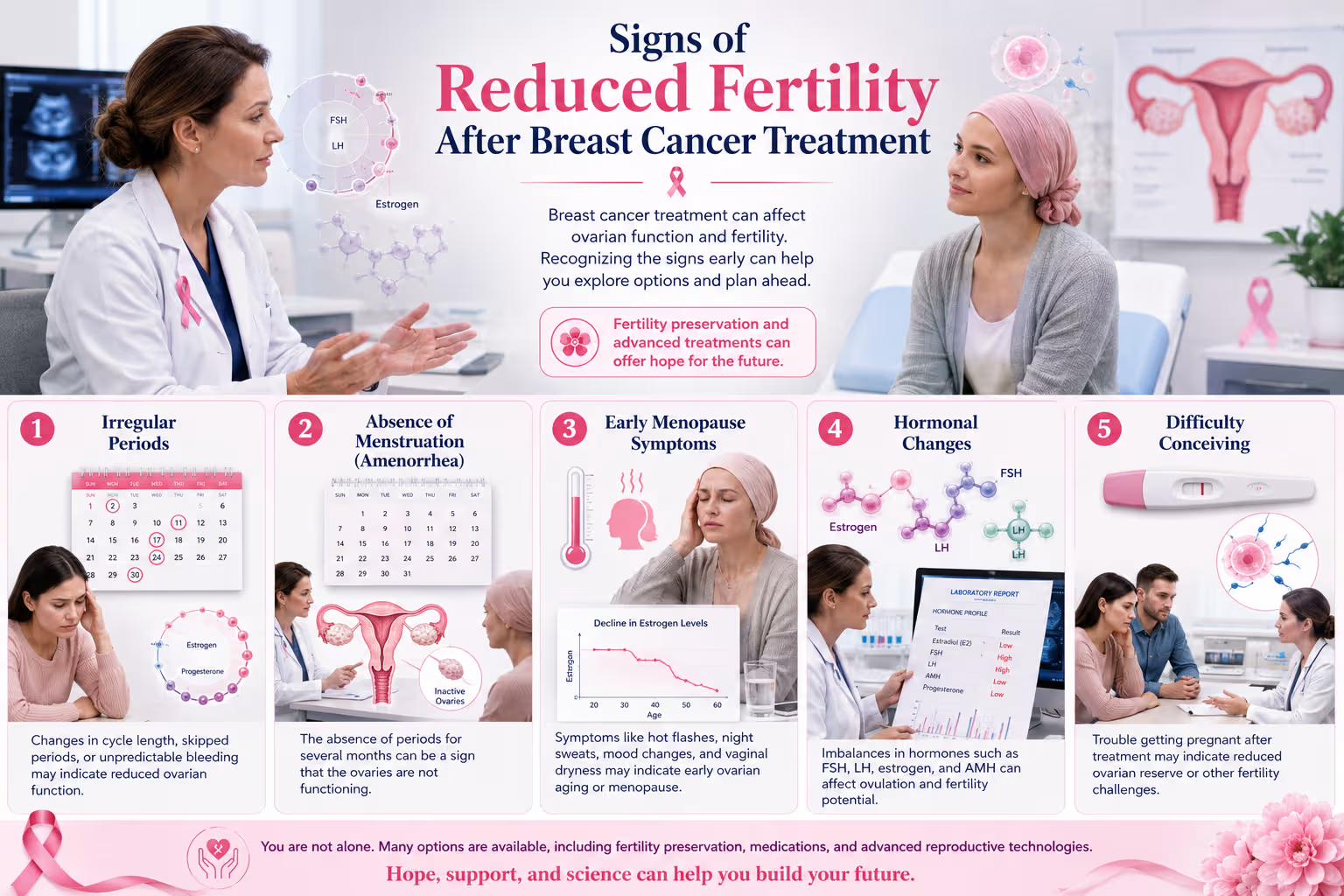
Signs of Reduced Fertility After Breast Cancer Treatment
Following treatment, women should monitor their bodies for signs that their ovarian function has been impacted:
-
Irregular Periods: Cycles that become significantly longer, shorter, or unpredictable.
-
Absence of Menstruation (Amenorrhea): If periods do not return within a year of completing chemotherapy.
-
Early Menopause Symptoms: Hot flashes, night sweats, and vaginal dryness.
-
Hormonal Changes: Significant drops in Estrogen or Anti-Müllerian Hormone (AMH) levels.
-
Difficulty Conceiving: Inability to get pregnant after six months of unprotected intercourse (for women over 35).
Fertility Preservation Options Before Treatment
The most critical window for preserving fertility is before the first dose of chemotherapy or the first surgical intervention. Modern reproductive technology offers several lifelines.
Egg Freezing (Oocyte Cryopreservation)
This is currently the “gold standard” for single women.
-
The Procedure: A woman takes hormone injections for about 10–12 days to stimulate the ovaries to produce multiple eggs. These eggs are then surgically retrieved and frozen.
-
Success Rates: Success depends on the age at the time of freezing and the number of eggs retrieved.
Embryo Freezing
For women in stable relationships, embryos can be created using the partner’s sperm and then frozen (cryopreserved). This method generally has a slightly higher success rate for future pregnancy than egg freezing alone.
Ovarian Tissue Freezing
An emerging and highly specialized option, particularly for prepubescent girls or women who cannot delay treatment even by two weeks. A small piece of the ovary is removed and frozen, to be re-implanted after cancer treatment.
Ovarian Suppression (GnRH Agonists)
Drugs like Leuprolide or Goserelin are used to put the ovaries into a “dormant” state during chemotherapy. The theory is that dormant ovaries are less susceptible to damage from chemo drugs.
Comparison of Fertility Preservation Options
| Option | Who it’s for | Timing Required | Success Potential |
| Egg Freezing | Single women / those preferring autonomy | 2 weeks | High (age-dependent) |
| Embryo Freezing | Women with a partner/sperm donor | 2 weeks | Very High |
| Ovarian Tissue Freezing | Urgent cases / young patients | Immediate (1-2 days) | Experimental but promising |
| Ovarian Suppression | During Chemotherapy | No delay needed | Moderate/Supportive |
Step-by-Step Fertility Planning Before Breast Cancer Treatment
If you have been diagnosed, follow this roadmap to ensure your reproductive goals are prioritized:
-
Step 1: Discuss Fertility Goals: Immediately inform your oncologist that future pregnancy is important to you.
-
Step 2: Consult a Fertility Specialist: Your oncologist should refer you to a reproductive endocrinologist (fertility doctor) within 24–48 hours of diagnosis.
-
Step 3: Assess Ovarian Reserve: Undergo blood tests (AMH) and an ultrasound (Antral Follicle Count) to see your current egg supply.
-
Step 4: Choose a Preservation Method: Decide between egg, embryo, or tissue freezing based on your personal circumstances.
-
Step 5: Begin Cancer Treatment: Once the eggs or embryos are safely stored, you can proceed with chemotherapy or surgery with peace of mind.
Can You Get Pregnant After Breast Cancer Treatment?
Many women wonder if the cancer will return if they get pregnant, or if the treatment has made it unsafe to carry a baby. The answer for most women is yes, pregnancy is possible and generally safe.
When is Pregnancy Safe?
Most doctors recommend waiting at least two years after finishing treatment before trying to conceive. This “waiting period” is important because:
-
The risk of cancer recurrence is highest in the first two years.
-
It allows the body to clear chemotherapy drugs.
-
It provides time for ovarian function to stabilize.
Is Pregnancy After Breast Cancer Safe?
Research, including the landmark POSITIVE Trial, has shown that for many women with hormone-receptor-positive breast cancer, temporarily pausing hormone therapy to attempt pregnancy did not increase the short-term risk of recurrence.
Breastfeeding After Breast Cancer Treatment
Breastfeeding is another common concern. Can you nurse a child after having breast surgery or radiation?
-
Following Surgery: If you have had a lumpectomy, you may still be able to breastfeed from that breast, depending on how much ductal tissue was removed. If you have had a unilateral mastectomy, you can successfully breastfeed from the remaining healthy breast.
-
Following Radiation: Radiation can damage the milk-producing glands, making it difficult or impossible for that specific breast to produce milk.
-
Safety: There is no evidence that breastfeeding increases the risk of cancer recurrence. However, you cannot breastfeed while taking chemotherapy or hormone therapies like Tamoxifen, as these drugs pass through breast milk.
Emotional and Psychological Impact of Fertility Concerns
Dealing with a cancer diagnosis is hard enough; adding the fear of infertility can be overwhelming. Many women experience:
-
Grief: Mourning the loss of “natural” parenthood.
-
Anxiety: Feeling pressured to make massive life decisions in a matter of days.
-
Relationship Strain: Navigating these choices with a partner under extreme stress.
Coping Strategies:
-
Counseling: Seek a therapist who specializes in oncology or infertility.
-
Support Groups: Connect with organizations like Young Survival Coalition to talk to others who have walked this path.
Questions to Ask Your Oncologist Before Starting Treatment
When meeting with your medical team, use these questions as a guide:
-
How likely is my specific chemotherapy regimen to cause permanent menopause?
-
Can we delay treatment for two weeks so I can freeze my eggs?
-
Are there “fertility-sparing” chemotherapy options available for my stage of cancer?
-
Will you use GnRH agonists (ovarian suppression) during my chemo?
-
Is there a Breast Cancer Specialist in Lucknow you recommend who focuses on young women’s health?
Fertility Preservation Awareness in India
In India, the conversation around breast cancer and fertility is evolving. Historically, the focus was solely on survival. However, as survivorship rates increase, the “quality of life” after cancer—which includes the ability to have a family—has become a priority.
In cities like Lucknow, access to advanced oncofertility care is expanding. Dr. Farah Arshad, a dedicated Breast Cancer Specialist in Lucknow, emphasizes that “surviving cancer is the first victory, but thriving afterward is the ultimate goal.” She advocates for early fertility counseling so that patients can make empowered decisions before treatment begins, ensuring that the life they save is the life they want to live.
FAQs – Breast Cancer Treatment and Fertility
1. Can breast cancer treatment make you infertile?
Yes, chemotherapy and certain hormone therapies can damage the ovaries or stop egg production, leading to temporary or permanent infertility.
2. Can I get pregnant after chemotherapy for breast cancer?
Many women do. However, it depends on your age, the type of chemo used, and how your ovaries recover. Consulting a fertility specialist is recommended.
3. Is pregnancy safe after breast cancer treatment?
Generally, yes. Most studies show pregnancy does not increase the risk of recurrence, though timing should be discussed with your oncologist.
4. How long should I wait to get pregnant after breast cancer?
The standard recommendation is usually 2 years, but this varies based on your specific cancer type and treatment plan.
5. Does radiation therapy affect fertility?
Radiation for breast cancer usually does not affect fertility because it is localized to the chest.
6. What is the best fertility preservation option?
Embryo or egg freezing are considered the most successful methods for most women.
7. Can I freeze my eggs before chemotherapy?
Yes, and it is highly recommended to do so if you wish to have biological children in the future.
8. Does hormone therapy delay pregnancy plans?
Yes, because you cannot be pregnant while taking drugs like Tamoxifen, you may need to wait 5–10 years or discuss a “temporary pause” with your doctor.
9. Can breast cancer survivors have healthy babies?
Absolutely. There is no evidence that previous breast cancer treatment leads to higher rates of birth defects in children.
10. When should I discuss fertility preservation with my doctor?
Immediately upon diagnosis, ideally before any surgery or chemotherapy begins.
Conclusion
A breast cancer diagnosis is a heavy burden, but it does not have to mean the end of your dreams for a family. While it is true that breast cancer treatment may affect fertility, infertility is not an inevitable outcome for every woman.
With the advent of egg and embryo freezing, ovarian suppression, and better-timed treatment protocols, the path to parenthood remains open for many survivors. The most critical factor is early intervention. Timely discussions with cancer and fertility specialists can drastically improve your future reproductive choices.
If you or a loved one is navigating a diagnosis and has concerns about future fertility, do not wait. Consult Dr. Farah Arshad, an experienced Breast Cancer Specialist in Lucknow, to discuss a personalized treatment plan that prioritizes both your health and your future family goals.
CTA
A breast cancer diagnosis brings many questions about the future. Understanding your options for fertility preservation before treatment begins can make a significant difference in your long-term reproductive health.
If you have been diagnosed with breast cancer and are concerned about fertility, contact Dr. Farah Arshad, a leading Breast Cancer Surgeon in Lucknow, for a comprehensive consultation on personalized treatment planning and fertility preservation.